Retake
V3) Hypotention in a patient with acute onset tearing chest pain
Review the Learning Outcomes, Hx, PE and Labs, and begin the module with your Provisional Diagnosis. Keep hitting "Next" to move through the module.
Learning Outcomes
- Articulate your relationship with the consulting diagnostic radiologists in the evaluation of a patient with chest pain.
- Review the DDx considerations in a patient with chest pain.
- Identify the spectrum of imaging findings in appropriate modalities for evaluating a patient with chest pain.
History
An 82-year-old female with 80 pack year smoking history and uncontrolled hypertension presents due to new onset shortness of breath and severe, tearing chest pain radiating to the back.
Physical Exam
BP: 79/40 (SBP falls by 15 on inspiration), HR 120, RR 25, Temp 36.4, O2 saturation 100%. CV: Muffled heart sounds. Otherwise, fast rate and regular rhythm. Distended neck veins bilaterally.
Labs
EKG: alternating and overall decreased QRS amplitude in all leads. No ST changes.
Provisional Diagnosis
Select the Dx you believe is most appropriate
This patient with significant smoking history, uncontrolled hypertension, and severe acute chest pain radiating to the back likely has an aortic dissection. The hypotension, distended neck veins, muffled heart sounds (Beck’s triad), electrical alternans, and lowered EKG voltage are all suggestive of cardiac tamponade, which may be secondary to the aortic dissection.
Well done. You were correct
Potential Acuity
What is your assessment of the likely acuity for this patient?
Well done. You were correct
The patient requires emergent workup as her potential condition is immediately life threatening.
First Imaging Study
What is the first imaging study you will order?
A chest CTA provides good non-invasive evaluation of the aorta and also detect suspected tamponade.
Well done. You were correct
Pertinent Imaging Observations
Click on the links below to view images from the study, and assess these key findings as best you can.
Chest CTA
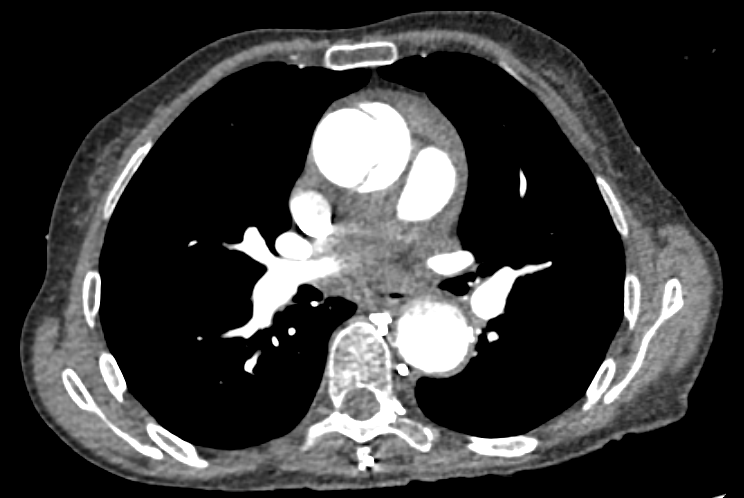
There is a dissection of the ascending aorta
The dissection flap is visible in the ascending aorta.
There is a dissection of the descending aorta
The dissection flap is visible in the descending aorta in this contrasted study.
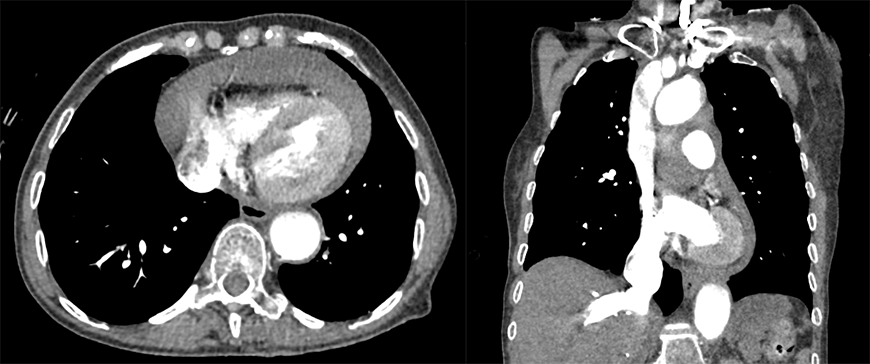
There is pericardial tamponade
There is pericardial tamponade as evidenced by the blood in the pericardium, the compressed ventricles, and reflux of contrast into the liver. In this case, the tamponade is secondary to the ascending aortic aneurysm.
View the full study if you'd like to take a look yourself.
Second Imaging Study
What is the next imaging study you will order?
The diagnosis is confirmed with the chest CTA.
Well done. You were correct
What is your Diagnosis now that you have seen the imaging results?
The patient’s clinical signs, symptoms, and imaging findings are consistent cardiac tamponade secondary to hemopericardium from aortic dissection. The Stanford classification is type A as it involves the ascending aorta. A type B dissection would only involve the descending aorta.
Current Acuity
Initially, you selected and we suggested acuity.
Has your concern for this patient changed?
The patient requires emergent evaluation and management as their condition is immediately life threatening.
Assessment and Plan
Please provide your assessment and plan for this patient
The patient is an 82-year-old female presenting with cardiac tamponade secondary to a Stanford Type A aortic dissection. Cardiothoracic surgery should be emergently consulted for evaluation of surgical repair.
Lessons Learned: Cardiac tamponade occurs when a pathologic structure or fluid in the pericardial cavity results in impaired cardiac output. It commonly occurs secondary to blood from an aortic dissection leading to pericardium, as seen in this case. The diagnosis can be confirmed with echocardiography, MRA, CTA, or CT with IV contrast.
Socioeconomic Factors: Patients with lower socioeconomic status were found to have reduced short- and long-term survival following aortic dissection.
That's the end of the module! Once you've reviewed the video(s), you can click here for another case challenge.
Contributors:
Kevin Pierre, MD - Editor
Robbie Slater, MD - Supervising Editor
Bayar Batmunh, MS - Coordinator
Next


{kind=link}
{kind=link}